Nominate an FCB Health & Dental Provider
Fill out this form.
Save $465-$2,100/year On All Your
Health & Dental Needs
Save $465-$2,100/year On All Your Health & Dental Needs

We are Canada's 1st non-profit health & dental savings plan.
✅ Create your account & start saving 20% - 30% by joining the FCB Health Network.
✅ Create your account & start saving
20% - 30% by joining the FCB Health Network.
⭐️⭐️⭐️⭐️⭐️ trusted by 3,200+ Canadians 🇨🇦
We are Canada's 1st non-profit health & dental savings plan.
⭐️⭐️⭐️⭐️⭐️ trusted by 3,200+ Canadians 🇨🇦
So far, Canadians have saved a combined $220,000 on all their treatments
So far, Canadians have saved a combined $220,000 on all their treatments






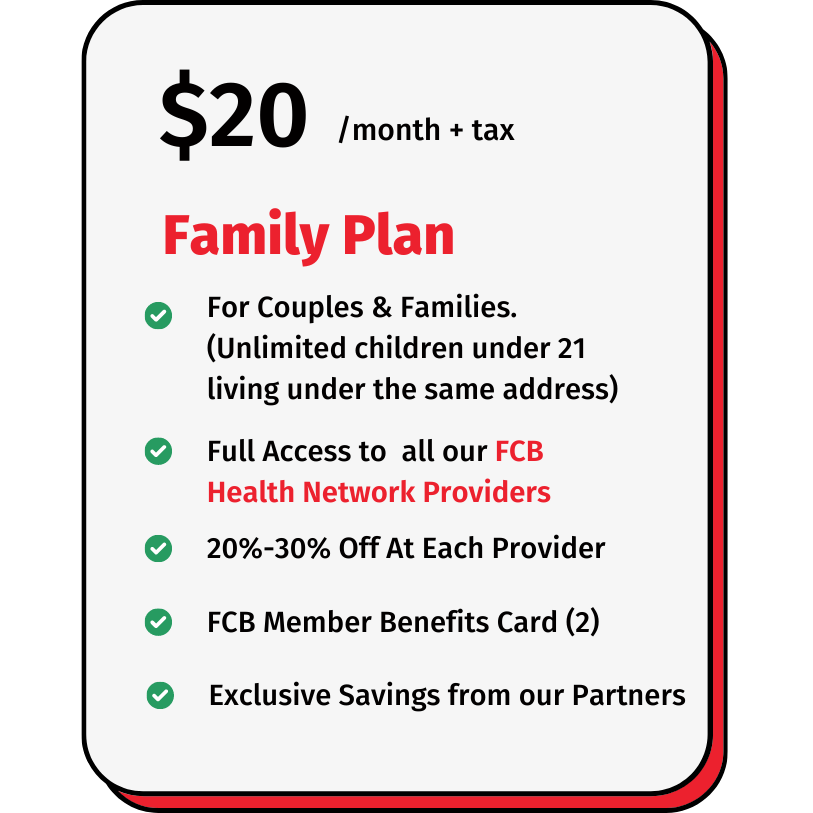
Our Member Pricing


Maximize Your Health,
Minimize Your Costs.

Clinical and corporate governance for the FCB Health Network
